Autism spectrum disorder: an update for GPs

Child mental health
Autism spectrum disorder (ASD) can be associated with comorbid mental health problems such as anxiety, attention deficit hyperactivity disorder and depression. GPs have key roles in recognising early signs of ASD and referring for specialist assessment, providing timely support to the person with ASD and their family, and in assisting with co-ordinating therapists and specialist support.
- About one in 100 children in Australia are born with autism spectrum disorder (ASD).
- Signs of communication, social and behavioural disturbance at 12 to 24 months of age can be red flags for ASD.
- ASD is a lifelong condition that can be associated with the emergence of comorbid mental health problems such as anxiety, attention deficit hyperactivity disorder and depression.
- GPs have a key role in recognising early signs of ASD and referring these children for specialist assessment.
- GPs also have the important roles of reviewing specialist- prescribed medication and supporting highly stressed families.
- Deterioration in behaviour might indicate acute illness in a person with ASD. Medical review is critical if there is a sudden change in behaviour as this may be due to a simple medical problem such as an ear infection.
Picture credit: © Amelie-Benoist/BSIP/Medical Images Models used for illustrative purposes only
In Australia, about one in 100 children are born with an autism spectrum disorder (ASD).1 This diagnosis is made when the child has difficulty understanding, learning and using language and relating socially to others and also has repetitive play, interests and behaviour. ASD emerges in early infancy, and the diagnosis can be reliably made from about 2 years of age.
The terms ‘autistic disorder’ (also known as ‘autism’) and ‘Asperger’s syndrome’ (also known as ‘Asperger’s disorder’) have been used in the past. In 2013, the American Psychiatric Association revised the diagnostic criteria, and the new term ‘autism spectrum disorder’ has now replaced these terms.2
GPs should be knowledgeable about the early signs of ASD, understand the importance of early intervention and be able to help parents contact early childhood intervention services.
Diagnosis of ASD
Parents who are worried about their child’s development and behaviour often seek help from an early childhood professional. A thorough and detailed assessment provides information about the child’s behaviour and development. Having a diagnosis of ASD is important, helping to:
- create a pathway for help and treatment
- target areas of need as well as strengths to build on
- access ASD-specific disability services and Medicare funding.
Diagnosis of ASD relies upon matching the child’s behaviour and development with diagnostic criteria. The diagnosis is made by a multidisciplinary diagnostic team according to specific criteria. The most recent criteria are those in the Diagnostic and Statistical Manual of Mental Disorders, 5th ed (DSM-5) of the American Psychiatric Association.2 DSM-5 guides the team in diagnosing ASD according to a specific number of symptoms that must be both present in early childhood and impairing everyday functioning. These symptoms are listed in Box 1.
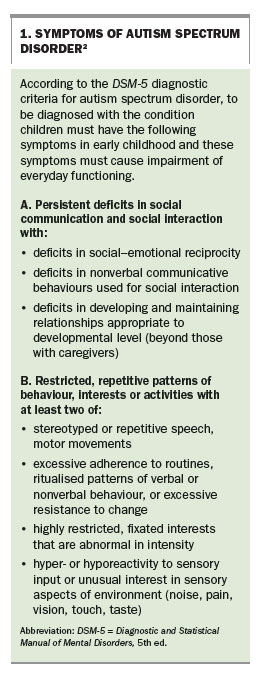{kind=link}
DSM-5 has three levels of severity of ASD, and emphasises that these levels should not be used to assess eligibility for services. The levels are:
- requiring ‘very substantial support’
- requiring ‘substantial support’
- requiring ‘support’.
In Australia, ASD assessment guidelines have been developed in the past that advocate a multidisciplinary approach to assessment using DSM-5 criteria. The Co-operative Research Centre for Living with Autism (Autism CRC) is undertaking a project to develop a national guideline for ASD diagnosis in this country. The goal is that this national guideline will define a diagnostic process that is rigorous, accessible, client-centred, clinically acceptable, effective, efficient and equitable for individuals being assessed for autism.3
A multidisciplinary assessment team is usually comprised of a paediatrician or child psychiatrist, speech pathologist, occupational therapist, psychologist and special educator. The team is not necessarily co-located for a single assessment; for example, the speech, language and cognitive assessments may be performed and reports written for the family to take to the appointment with the child psychiatrist or paediatrician, who will then make the diagnosis after gathering all the assessment information. Assessment should include:
- medical assessment, including tests for known causes of developmental delay and also hearing, vision and blood tests
- an interview to find out about the child’s early developmental and family history
- observation of the child’s behaviour and interactions (e.g. using the Autism Diagnostic Observation Schedule)
- developmental/cognitive assessment using appropriate standardised assessments
- language assessment (expressive, receptive and pragmatic language)
- assessment of emotions and behaviour, including parent- or teacher-completed checklists
- assessment of sensory problems, adaptive functioning, motor planning and co-ordination
- observation and reports from parents/caregivers, teachers and others who know the child well, to give a broad picture of each child.
Children with ASD present differently depending on their current symptoms, their cognitive ability and their educational and life experiences. IQ scores of children with ASD typically show a scattered pattern of performance, with deficits in verbal sequencing and abstraction skills, but with higher success in skills requiring rote memory, immediate memory or physical manipulation and visual–spatial skills (such as block design and object assembly). The IQ profiles of children with ASD who have better language skills and no history of delayed language often show strengths in verbal IQ and poorer nonverbal IQ (such as puzzles, sequencing and block design). The high-performing skills on a child’s IQ test may be the basis of so-called ‘islets of ability’. Some children with ASD show unusual abilities such as profound musical skills or exceptional cognitive skills – ‘savant skills’.
Research has shown that most people diagnosed with ASD in early childhood continue to have ASD symptoms in later life.4-6
Comorbidity
Common comorbid conditions in children with ASD include:
- developmental delay/intellectual disability
- anxiety and mood disorders
- communication disorders
- attention deficit disorders
- epilepsy.
Comorbid conditions may be related (e.g. there is an increasing likelihood of the onset of epilepsy in children with ASD) or they may be independent of each other (e.g. the child has diabetes and ASD).7
Early signs of ASD
Signs of ASD may be apparent in infancy but are often more obvious after the age of 2 years. Most parents of children with ASD notice differences in their child’s development and behaviour very early, sometimes before the child has turned 2 years of age. The five behaviours that are ‘red flags’ for autism are listed in Box 2.8 The presence of any of these red flags does not mean the child definitely has ASD, but a child showing these behaviours should be assessed by professionals knowledgeable about ASD. The red flags are increasingly being recognised by GPs, maternal and child health nurses, early childhood educators and allied health clinicians.
{kind=link}
Although it is known that the symptoms of ASD begin during early childhood, there is limited evidence about when symptoms actually start and their potential severity.9 Behaviours that are early indicators of ASD include those listed in Box 3.10-13
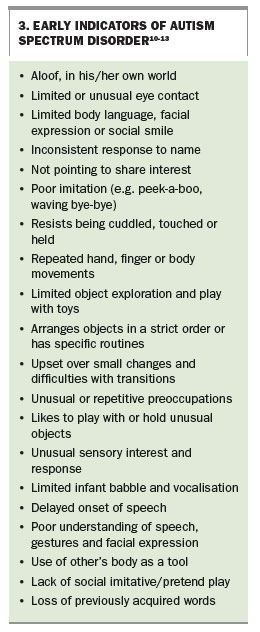{kind=link}
Regression in ASD
Loss of previously acquired skills, or regression, is reported in 20 to 33% of children with ASD and can include loss of words, vocalisations, nonverbal communication, social interaction skills, imitation or pretend play. The common time for loss of skills is reported as about 18 to 21 months.14
The pattern of symptoms in regression has led to suspicions that postnatal environmental factors such as immunisation with the measles–mumps–rubella (MMR)vaccine trigger autism. Although reports of a possible link between vaccination and autism began in the 1980s, no causal link has been confirmed (see later discussion of ASD and immunisation).15-17
Causes of ASD
ASD has no single known cause. Given its complexity and the fact that symptoms and severity vary, there are probably many causes, including genetic and environmental risk factors.
Genes and environment
Theories about what might cause ASD have changed over the past 60 years. In some families, there appears to be a pattern of ASD or other disabilities. It also appears that some children are born with a susceptibility to autism, but researchers have not yet identified a single ‘trigger’ that causes autism to develop.18
Evidence supporting a significant genetic contribution to ASD has been increasing over the past few decades, but what causes or increases the risk for ASD is not yet understood.19 Studies have shown that among identical twins, if one child has ASD, then the other will be affected about 98% of the time; and in nonidentical twins, if one child has ASD, then the other is affected about 53% of the time.20
The patterns of genetic inheritance are complex, with the involvement of multiple genes rather than a simple dominant, recessive or X-linked gene.19 Several chromosome regions are likely to contain risk genes for ASD, but no gene has been unequivocally identified to date.21
Research has begun to show that environmental factors may also involve some genetic susceptibility. A recent study has shown that at an individual level, the risk of autism increases according to how close a person is genetically to relatives with autism.22
Other possible causes
About 10% of people with ASD have known potentially causative medical conditions, including Fragile X syndrome, tuberous sclerosis, congenital rubella syndrome and untreated phenylketonuria. A small proportion of children who are born prematurely or with low birthweight are at greater risk of ASD, and advanced paternal and maternal age, growth restriction and newborn hypoxia are also associated with an increased risk of ASD.23-25
ASD and immunisation – no link
Over the past decade there has been considerable discussion, publicity and research regarding whether there is a link between autism and immunisation. As mentioned earlier, comprehensive studies have provided no evidence to support a link between MMR vaccination and ASD;15-17 previous studies suggesting a causal link were found to be seriously flawed. There is also no evidence to suggest that any other childhood vaccine may increase the risk of ASD or to support an association between vaccine preservatives such as thimerosal (which contains ethylmercury) and ASD.26
Risk of ASD if relatives affected
In the general population worldwide, ASD affects about one in 100 children.27 As previously mentioned, a recent studyprovided measures of individual risk for children who have a relative with ASD: children are 10 times more likely to develop ASD if they have a sibling with ASD, three times more likely if they have a half-brother or sister with ASD, and two times more likely if they have a cousin with ASD.22 There are no differences in relative risk between genders.
Increase in rate of ASD
There has been much discussion as to why the prevalence of autism has been steadily increasing. One reason is the change in diagnostic criteria in 1994. At that time, the diagnostic criteria for autism expanded to include children who were not previously considered to be ‘on the spectrum.’
Studies have shown that, despite this change in diagnostic criteria, the prevalence of diagnosed cases of ASD is now much higher than expected. Many researchers believe the increase in the number of cases of autism worldwide may also be due to a combination of genetic and environmental factors described above.
Changes in ASD over time
In people with ASD, there is generally a pattern of improvement from childhood to adolescence to adulthood, with symptoms usually decreasing over time.28
The preschool years
A young child with ASD is often disinterested in others, does not understand the feelings of other people, their speech may be absent or delayed and they may be upset by even small changes and have a range of sensory sensitivities. Special interests and repetitive body movements may become more noticeable after 3 years of age.
Many parents with a child with ASD find the child’s preschool years the most difficult to manage but, with early intervention, education and support, improvement can be expected. Early intervention that improves learning abilities can lead to better social and language skills in adolescence and early adulthood.2 For example, if a preschool-aged child is able to develop skills such as functional play and is responsive to others, can engage in joint attention and make social requests, they are more likely to have better language skills in the future.28
The primary school years
Some parents report that the primary school years are more settled than the preschool years for their child with ASD and the whole family, particularly when the transition to school has been carefully planned and there is ongoing support from the school. With education and understanding, primary school-aged children may become more socially responsive and communication skills can increase.
Other parents, however, find that their child with ASD develops behavioural difficulties and anxiety from coping with change and social demands once they are out and about in the social world of school and peers. Preoccupations or special interests may also increase at this time. Helping to build stronger social skills during middle childhood has been shown to lead to improvements during adolescence.29 Writing social stories together with the child with ASD that tell him/her how to behave and what to say in social settings, joining social skills training groups where there are opportunities to role play and practise social interaction skills, and having opportunities to mix with peers in supervised, structured settings are all helpful for children with ASD.
Adolescence
Young people with ASD experience the same changes and growth in body and mind as other adolescents but their ASD continues to affect the core areas of social interaction, communication and behaviour. GPs can play an important role in helping the adolescent with ASD and their family to prepare for the changes in the young person over the next few years.
Some parents have described more social interaction, less repetitive behaviours, better daily living skills and more emotional responsiveness in their teenage sons and daughters with ASD. High-functioning adolescents with ASD (normal IQ range) have been reported to show more improvement than adolescents with ASD and intellectual disability.29 For other parents, adolescence in their child with ASD can bring an increase in anxiety, tension, mood disturbance and social withdrawal, with a focus on preoccupations such as electronic games. This may be due to a combination of the development of some degree of insight as well as hormonal and developmental changes.
For most adolescents, the bodily changes that they experience at this time have a significant effect on how they feel about themselves. As most young people with ASD do not like change, these physical changes can be overwhelming. Preparing adolescents for the changes that will occur can minimise confusion and fears about their changing bodies. Ideally, education about puberty needs to start well before it is actually occurring to be most beneficial to each young person.
Adolescents with ASD are also likely to need to be taught about growth and development, personal hygiene and sex education, in a direct, simple and clear manner at their level of comprehension. As young people with ASD usually have better visual skills than language skills, it makes sense that teaching around the issues of puberty and sexuality will be more easily understood if pictures and visual supports are used; this is so even for the higher functioning adolescents. Opportunities for social involvement with peers leads to more social awareness and better daily living skills in adolescents with ASD. Focusing intervention programs in the individual’s area of social skills is important.29
Television, video games and social media
Parents may communicate that they are worried about their adolescent son or daughter with ASD, saying, for example, ‘He is spending hours alone in the bedroom with the computer. Do we tell him to come out and be with the family or leave him alone?’ Many parents face this dilemma with their teenage sons and daughters with ASD. Are the adolescents avoiding social interaction or making friends and learning social skills online in a nonthreatening way?
Screen-based media such as television, video games, computer games and electronic social media (including email, text messages and online social networking sites like Facebook and video-sharing sites like YouTube) are an increasingly popular tool for entertainment and social connection among typically developing children and adolescents. Communicating online through email, instant messaging and text messaging can offer opportunities for social interaction in a format that does not require attention to nonverbal cues such as gestures, facial expressions or voice nuances. Computer technology provides a more controlled and predictable environment than face-to-face interaction, and this can be particularly desirable for adolescents with ASD who want to be in touch with friends but do not like to be physically face to face with them.
Recent research, however, has found that preoccupation with media appears to be a clinically significant problem. Adolescents with ASD were reported by parents to spend 62% more time watching television and playing video games than all nonscreen-daily activities combined.30 In contrast, children with ASD also spent little time using social media or socially interactive video games.30
Two useful take-home messages regarding screen-based media are:
- care must be taken to develop strategies for building generalisation from solitary screen media formats to real-world social situations
- communicating online can be helpful for adolescents with ASD who want to interact with peers but find it difficult to manage face to face; however, time limits should be set, and a range of opportunities for ‘offline’ social interaction also offered.
Adulthood
Although the outcome for adults with ASD has improved over recent years, many remain dependent on others for support. Those with an intellectual disability may have more ASD symptoms and behavioural difficulties than those without intellectual disability.31 Some adults achieve relatively high levels of independence but for most the challenges continue, including living alone, having close friends and being in permanent employment. Appropriate vocational training and supported work, recreation and accommodation, and the development of wider social support networks are ongoing needs of adults with ASD. Recognition, monitoring and treatment of physical and mental health problems are also necessary.
The GP who has developed a relationship, sometimes over many years, with the person with ASD and their family is ideally placed to assist the transition from paediatric to adult services. To ensure the transition is as smooth as possible it is essential that not only the medical history, including general health, mental health and wellbeing, of the person with ASD is passed on to adult service providers but also information about recent successful treatment and management strategies.
Treatment options for children with ASD
Several interventions are available to help a child with ASD but there is no specific treatment that can cure ASD.32 The goal of intervention is to maximise the child’s ability and skills by supporting their development and learning (Figure).
{kind=link}
A diagnosis of ASD brings a multitude of questions about what to do next. Parents need to make important decisions about their child’s education and treatment. Treatment should begin as early as possible and be tailored to the child’s profile of symptoms, strengths and needs. A variety of evidence-based interventions are more likely to promote development, improve behaviour and reduce the stress experienced by the child and family. Some common treatment approaches are outlined below; more information can be found on the Raising Children Network website supported by the Australian Federal Government.
Educational interventions
Children with ASD often respond well to highly structured educational programs that are based on understanding the culture of ASD, developing an individual person- and family-centred plan for each student, structuring the physical environment to enhance learning, using visual supports to make the sequence of daily activities predictable and understandable, and using visual supports to make individual tasks understandable. An example of such a program is the TEACCH (Treatment and Education of Autistic and Related Communication-Handicapped Children) program.33 Successful programs include parents and professionals working together to improve social skills, communication and behaviour in daily activities.
Behaviour-based interventions
Preschool children with ASD who receive individualised behavioural interventions can make good progress. Intensive early behavioural interventions that target a range of essential skills that define or are associated with ASD (e.g. communication, social and pre-academic/academic skills) can be helpful. These interventions are also described as applied behaviour analysis, early intensive behavioural interventions or behavioural inclusive programs.34,35
Therapy-based interventions
A therapy-based approach to intervention for ASD is the use of specific therapies to target specific difficulties (social, behavioural and/or language). Some programs focus on reducing problem behaviours and teaching new skills, and others focus on teaching children how to act in social situations or how to communicate better with others (e.g. the Hanen Program [language communication] and the Picture Exchange Communication Program [visual communication]).36,37
Family-based interventions
There is no doubt that the family of the child with ASD needs help and support. Stressors can be present whatever the severity level of the child’s ASD symptoms. It should be remembered that parents of children with high functioning ASD might also have high levels of stress.
Treatment therefore should not focus exclusively on the child with ASD. Parents need to learn effective strategies for coping with their own distress. This is particularly important if a parent also has the condition. Parents and other family members can learn how ASD affects the child and how to play and interact with them in ways that promote social interaction skills, as well as how to manage problem behaviours and how to teach daily living skills and communication. Examples of programs that can improve child outcomes and reduce family stress are the Triple P Positive Parenting Program and Preschoolers with Autism.38,39
Medical interventions
Although there are no evidence-based pharmacological treatments for ASD, some drugs can improve certain symptoms of emotional and behavioural difficulties associated with ASD. Neuroleptics (e.g. risperidone, aripiprazole) can reduce disruptive, irritable and aggressive behaviours but problematic side effects, particularly weight gain and metabolic syndrome, are common. Selective serotonin reuptake inhibitors (e.g. fluoxetine, sertraline) and tricyclic antidepressants (e.g. imipramine, clomipramine) can reduce comorbid symptoms of anxiety, obsessive–compulsive disorder and depression. Attention deficit hyperactivity syndrome is often associated with ASD (30 to 50% of cases) and can be treated with stimulant medication, although side effects are common.
Parents and professionals need to make informed decisions about treatment options for children. However, it can be difficult to work out whether a treatment being considered for a particular child is known to be effective.
Parents should be encouraged to ask questions and think critically about treatments for their child with ASD.40 For example:
- Will the treatment result in harm to my child (physical or psychological)?
- Is the treatment developmentally appropriate for my child?
- How might failure of the treatment affect my child and family?
- Has the treatment been validated scientifically?
- Will the treatment be integrated into my child’s current program or will it be extra time?
- What are the costs?
Particular points to remember to talk about with families include:
- beware of treatments that promise ‘cure’ and are said to work for all children with ASD
- for any treatment, baseline and follow-up evaluation of key symptoms using a behavioural checklist are necessary to demonstrate benefit
- regular health and dental checks are important. Current sleep patterns, diet and level of physical activity should be discussed.
Conclusion
Many families acknowledge that their GP is the first and most important contact for them and their child with ASD. GPs can provide a crucial role in early detection and ongoing review and support for individuals with ASD and their families. Over time, they get to know the family’s strengths and weaknesses and how best to support the various family members. Importantly, GPs are in a position to provide timely support, as and when needed, to the person with ASD and their family. They are also available to assist the family in the important task of co-ordinating therapists and specialist support.
MT
COMPETING INTERESTS: None.
References
- McDermott S, Williams K, Ridley G, Glasson E, Wray J. The prevalence of autism in Australia: can it be established from existing data? Report commissioned by the Australian Advisory Board on Autism Spectrum Disorders. 2007. Available online at: http://www.autismadvisoryboard.org.au/uploads/Autism Prevalence Study FINAL Feb 07.pdf (accessed April 2017).
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. (DSM-5) Arlington, VA: American Psychiatric Publishing; 2013.
- Autism CRC. National guideline for autism diagnosis in Australia. Available online at: https://www.autismcrc.com.au/national-guideline-autism-diagnosis-australia (accessed April 2017).
- Chawarska K, Paul R, Klin A, Hannigen S, Dichtel LE, Volkmar F. Parental recognition of developmental problems in toddlers with autism spectrum disorders. J Autism Dev Disord 2007; 37: 62-67.
- Moore V, Goodson S. How well does early diagnosis of autism stand the test of time? Follow-up study of children assessed for autism at age 2 and development of an early diagnostic service. Autism 2003; 7: 47-63.
- Stone W, Lee E, Ashford L, Brissie J, Hepburn S, Coonrod E, Weiss B. Can autism be diagnosed accurately in children under 3 years? J Child Psychol Psychiatry 2003; 40: 219-226.
- Amiet C, Gourfinkel-An I, Bouzamondo A, et al. Epilepsy in autism is associated with intellectual disability and gender: evidence from a meta-analysis. Biol Psychiatry 2008; 64: 577-582.
- Filipek PA, Accardo PJ, Ashwal S, et al. Practice parameter: screening and diagnosis of autism. Report of the quality standards subcommittee of the American Academy of Neurology and the Child Neurology Society. Neurology 2000; 55: 468-479.
- Ozonoff S, Iosif AM, Baguio F, et al. A prospective study of the emergence of early behavioral signs of autism. J Am Acad Child Adolesc Psychiatry 2010; 49: 256-266.
- Zwaigenbaum L, Bryson S, Rogers T, Roberts W, Brian J, Szatmari P. Behavioral manifestations of autism in the first year of life. Int J Dev Neurosci 2005; 23: 143-152.
- Yirmiya N, Charman T. The prodrome of autism: early behavioral and biological signs, regression, peri‐and post‐natal development and genetics. J Child Psychol Psychiatry 2010; 51: 432-458.
- Bryson SE, Zwaigenbaum L, McDermott C, Rombough V, Brian J. The Autism Observation Scale for Infants: scale development and reliability data. J Autism Dev Disord 2008; 38: 731-738.
- Bolton PF, Golding J, Emond A, Steer CD. Autism spectrum disorder and autistic traits in the Avon Longitudinal Study of Parents and Children: precursors and early signs. J Am Acad Child Adolesc Psychiatry 2012; 51: 249-260.
- Goldberg WA, Osann K, Filipek PA, et al. Language and other regression: assessment and timing. J Autism Dev Disord 2003; 33: 607-615.
- Honda H, Shimuzu Y, Rutter M. No effect of MMR withdrawal on the incidence of autism: a total population study. J Child Psychol Psychiatry 2005; 46: 572-583.
- DeStefano F. Vaccines and autism: evidence does not support a causal association. Clin Pharmacol Ther 2010; 82: 756-759.
- Mrozek-Budzyn D, Kieltyka A, Majewska R. Lack of association between measles-mumps-rubella vaccination and autism in children: a case-control study. Ped Infect Dis J 2010; 29: 397-400.
- Constantino JN, Todorov A, Hilton C, et al. Autism recurrence in half siblings: strong support for genetic mechanisms of transmission in ASD. Mol Psychiatry 2013; 18: 137-138.
- Gupta AR, State MW. Recent advances in the genetics of autism. Biol Psychiatry 2007; 61: 429-437.
- Tick B, Bolton P, Happé F, Rutter M, Rijsdijk F. Heritability of autism spectrum disorders: a meta-analysis of twin studies. J Child Psychol Psychiatry 2016; 57: 585-595.
- Yang MS, Gill M. A review of gene linkage, association and expression studies in autism and an assessment of convergent evidence. Int J Dev Neurosci 2007; 25: 69-85.
- Sandin S, Lichtenstein P, Kuja-Halkola R, Larsson H, Hultman C, Reichenberg A. The familial risk of autism. JAMA 2014; 311: 1770-1779.
- Kolevzon A, Gross R, Reichenberg A. Prenatal and perinatal risk factors for autism. Arch Ped Adolesc Med 2007; 161: 326-333.
- Lundström S, Hamworth C, Carlström E, et al. Trajectories leading to autism spectrum disorders are affected by paternal age: findings from two nationally representative twin studies. J Child Psychol Psychiatry 2010; 51: 850-856.
- Gardener H, Spiegelman D, Buka S. Perinatal and neonatal risk factors for autism: a comprehensive meta-analysis. Pediatrics 2011; 128: 344-355.
- Fombonne E. Thimerosal disappears but autism remains. Arch Gen Psychiatry 2008; 65: 15-16.
- Elsabbagh M, Divan G, Koh Y-J, et al. Global prevalence of autism and other pervasive developmental disorders. Autism Res 2012; 5: 160-179.
- Seltzer M, Krauss M, Shattuck P, Orsmond G, Swe A, Lord, C. The symptoms of autism spectrum disorders in adolescence and adulthood. J Autism Dev Disord 2003; 33: 565-581.
- McGovern CW, Sigman M. Continuity and change from early childhood to adolescence in autism. J Child Psychol Psychiatry 2005; 46: 401-408.
- Mazurek M, Wenstrup C. Television, video game and social media use among children with ASD and typically developing siblings. J Autism Dev Disord 2013; 3: 1258-1271.
- Howlin P, Goode S, Hutton J, Rutter M. Adult outcome for children with autism. J Child Psychol Psychiatry 2004; 45: 212-229.
- Francis K. Autism interventions: a critical update. Dev Med Child Neurol 2005; 47: 493-499.
- Mesibov GB, Shea V, Schopler E. The TEACCH approach to autism spectrum disorders. New York: Springer Science & Business Media; 2004.
- Keenan M, Kerr KP, Dillenburger K. Parents’ education as autism therapists: applied behaviour analysis in context. London: Jessica Kingsley Publishers; 2000.
- Reichow B, Barton EE, Boyd BA, Hume K. Early intensive behavioral intervention (EIBI) for young children with autism spectrum disorders (ASD). Cochrane Database Syst Rev 2012; 10: CD009260.
- Girolametto LE, Greenberg J, Manolson HA. Developing dialogue skills: the Hanen early language parent program. Semin Speech Lang 1986; 7: 367-382.
- Bondy A, Frost L. A picture’s worth: PECS and other visual communication strategies in autism (Topics in Autism). 2nd ed. Bethesda: Woodbine House; 2011.
- de Graaf I, Speetjens P, Smit F, de Wolff M, Tavecchio L. Effectiveness of the Triple P Positive Parenting Program on behavioral problems in children: a meta-analysis. Behavior Modification 2008; 32: 714-735.
- Brereton AV, Tonge BJ. Pre-schoolers with autism: an education and skills training programme for parents. Manual for clinicians. London: Jessica Kingsley Publishers; 2005.
- Freeman B. Guidelines for evaluating intervention programs for children with autism. J Autism Dev Disord 1997; 27: 641-651. MedicineToday 2017; 18(5): 42-48